
 ">
">
 ">
">
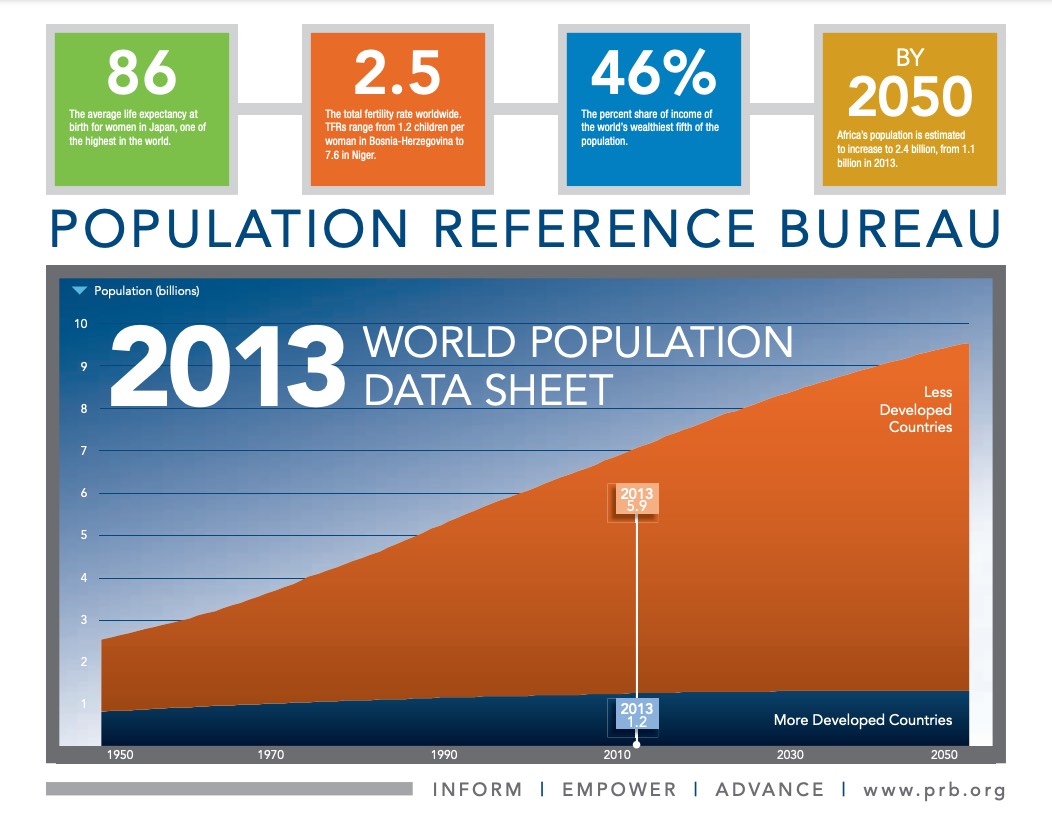
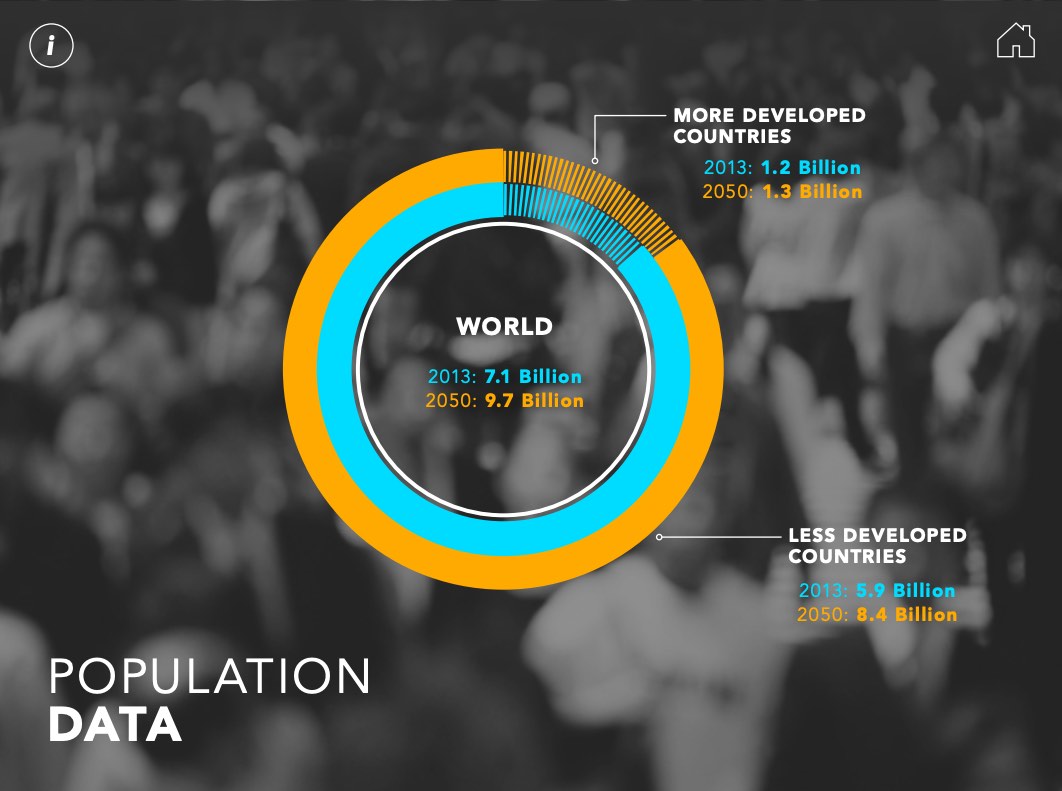
World population is expected to rise from 7.1 today to reach 8 billion by 2024, and virtually all this future growth will be concentrated in the world’s less developed countries, according to Carl Haub, PRB senior demographer and co-author of PRB’s 2013 World Population Data Sheet. The world’s poorest countries, which are predominantly in sub-Saharan Africa, will see the greatest increases, he said during a Sept. 13, 2013, webinar to mark the data sheet’s release. The 51 countries of sub-Saharan Africa are on a trajectory to grow from 170 million in 1950 to more than 2 billion in 2050, representing nearly a 12-fold increase in the span of 100 years. About two-thirds of this growth will occur over the next 40 years.
By contrast, industrialized countries as a whole will experience little or no population growth in this century, and some countries such as Japan and many in Europe are expected to decline. “For developed countries it’s the end of growth and the beginning of unprecedented aging,” he said. “There are very few potential parents moving up the age ladder.”
Webinar: 2013 World Population Data Sheet
However, the proportionately young populations in developing countries are “an engine of growth,” guaranteeing large numbers of young people entering their childbearing years annually. Sub-Saharan Africa is the “world’s youngest region” with 43 percent of the population younger than age 15, while in Europe 16 percent of the population is under age 15. And by 2050, sub-Saharan Africa’s under-15 population will decline but still make up about one-third of the population (34 percent), while Europe’s under-15 population will remain fairly static (15 percent) during the period.
The Demographic Divide
Haub compared Niger and the Netherlands to show the stark contrasts between less developed and more developed countries. Even though the two countries have almost the same population size today, Niger is projected to nearly quadruple its population from about 17 million today to 66 million in 2050. The Netherlands’ population will likely grow very slowly from 17 million to 18 million over that same time.
At the root of this “demographic divide” are differences in the average number of births per woman and the share of the population in their childbearing years. Niger’s total fertility rate of 7.6 lifetime births per woman is more than four times the Netherlands’ rate of 1.7 per woman. One-half of Niger’s population is younger than age 15, compared with 17 percent of the Netherlands’ population.
These population projections “assume that Niger’s birth rate will slowly come down” over the next 30 to 40 years, he noted. If women continue to average more than seven children each, Niger’s 2050 population total will be much higher.
Childbearing in Niger is shaped by deep poverty and a high level of infant deaths, explained Wendy Baldwin, PRB president and CEO, during the webinar. Per capita income in the Netherlands is 67 times greater than in Niger. The infant mortality rate is 51 deaths per 1,000 live births in Niger compared to 3.7 per 1,000 in the Netherlands. These rates translate into 43,000 infants dying before their first birthday each year in Niger, compared to just 650 in the Netherlands.
“It is when families feel that the children they have will survive that they begin to focus much more on controlling fertility and having fewer births,” Baldwin said. However, surveys show that about one-half of the women in some parts of sub-Saharan Africa who want to limit or space their children have no access to family planning. “I think there’s a real opening there to help women do what they would like to do and start to bring these high fertility rates down a bit,” she said.
Income Inequality
PRB’s 2013 World Population Data Sheet has a special focus on wealth and income inequality. Developing countries tend to have wide income gaps between rich and poor that are associated with dramatic differences in fertility and health. For example, in Uganda, women from the poorest fifth of families have twice as many children as those from the wealthiest fifth. In Nigeria, 86 percent of the poorest fifth of women in their reproductive years have no schooling, compared with 4 percent in the richest fifth, a “stunning difference,” said Baldwin.
“Schooling for women is very important; it is often a trigger for other investments in the family, especially in children,” she said. “We know that mothers’ education has a tremendous impact on child well-being, even on child mortality.” In Cambodia, children from the poorest fifth of families are three times more likely to die before reaching age 5 than their counterparts in the wealthiest fifth of families.
In the United States, the gap between the income share of the wealthiest and the poorest households is one of the widest among industrialized countries. In 2011, the poorest fifth of U.S. households received only 3 percent of total national household income while the richest fifth received 51 percent. This division is similar to Brazil’s, with the poorest fifth receiving 3 percent of national income and the richest fifth, 59 percent. “While the overall level of income is much higher in the United States, the disparity is about the same,” she noted.
But “it’s a different picture in India and Finland,” she pointed out. Although these two countries have very different standards of living, income distribution is much more equal. In Finland, the poorest fifth receive 10 percent of national income, while the richest fifth receive 37 percent. In India, the poorest fifth receive 9 percent of national income, while the richest fifth, 43 percent.
Q&A From PRB’s Webinar on the 2013 World Population Data Sheet
Carl Haub answered additional questions submitted during the webinar.
Q: Wow, wonderful presentation! An eye opener for demographic data analysis. I was expecting an example on what pertains to Ghana as in the case of Malawi. Can this type of analysis be done at the regional level to compare results, or is there a threshold? What software can be used for this type of analysis?
A: I imagine the same two pyramids for Ghana would show a similar overall pattern to Malawi, but less pronounced since Ghana has had a larger reduction in fertility. It could possibly be done for subnational regions that have fairly large populations, but there would be some limiting population size. The pyramids were run using SAS or SPSS, and the data user file from the Demographic and Health Survey.
Q: Do you consider spousal interaction as a determinant of fertility rate in developing and developed countries? I think women’s empowerment can explain a lot about high fertility in sub-Saharan Africa.
A: Yes, that is true. In the 2007 Zambia DHS, 54 percent of men said they believed women should have “the greater say alone or equal say with her husband” on the number of children to have, which means that 46 percent of men do not think so. Contraceptive use usually rises when women have a greater say in household decisions.
Q: How will the availability and politics of water affect populations, for instance in the Nile basin of east Africa?
A: I can’t claim expertise on a specialized topic such water, but there is a wealth of information on the subject. You may already be aware of it, but this World Bank resource cites many studies on the subject.
Q: Are there chances of decline in fertility in the fifth poorest in Nigeria?
A: Predicting the future course of fertility is a bit risky. But, we do have quite a bit to go on because Nigeria has had quite a few demographic surveys. Nationally, the total fertility rate (TFR) was reported as 5.7 in both the 2003 and 2008 Demographic and Health Surveys and in the 2011 Multiple Indicator Cluster Survey, indicating no declining trend. Among the poorest fifth, the TFR in those surveys was 6.5, 7.1, and 7.3, respectively, suggesting that the TFR is actually rising. The highest TFRs are routinely reported in the northeast and northwest regions at 6.7 to above 7. But regional rates also fluctuate, which may have more to do with the accurate reporting of births in the surveys than actual trends.
The use of modern family planning methods among the poorest fifth is by far the lowest in the country: among women married or in a union, the use of modern contraception was 3.6, 2.5, and 2.2 percent in the three surveys, respectively. Incidentally, 38 percent of women were in polygamous marriages, raising questions of women’s empowerment. Finally, only one-third of women in the poorest fifth with six or more living children said that they wished to cease childbearing.
Based on the above, the possibility of TFR decline among the poorest women in Nigeria seems remote.
Q: Thanks to the presenters for highlights on the 2013 world population data sheet. In one of the slides you showed the fertility trends in the United States comparing the white non-Hispanics with white Hispanics. How do the other subgroups such as African Americans and Asians compare with the white non-Hispanics?
A: By the way, the TFR for Hispanics in the webinar graph is for all Hispanics, not just white Hispanics. The TFRs for other groups is (2012 data): Black non-Hispanic: 1.899; American Indian/Alaska Native: 1.350; and Asian/Pacific Islander: 1.770
TFRs for 2011 and 2012 are given in the U.S. National Center for Health Statistics publication in Table 1 on page 23. Longer past trends are in in Table 4 on page 55 and in Table 8 on page 63, which detail on Hispanic origin.
Q: Do you see any patterns in fertility rates between the wealth quintiles in the United States?
A: Other than the fact that fertility has fallen more rapidly among the ethnic groups that are likely to be in lower income categories, I don’t know of any data from NCHS that addresses your question directly. There may be something in the Census Bureau’s Current Population Survey.
Q: You showed the Hispanic fertility rate higher than the non-white Hispanic rate. Is there a further breakdown of Hispanic foreign-born and Hispanic second-generation?
A: An excellent question. There’s a good chance the Current Population Survey includes “nativity” in their tables. If not, analysis of the age structure of Hispanics by nativity would be useful.
Q: Is there a cultural block against the terms “population control” or “family planning”?
A: There is, in my opinion, a definite cultural block against population “control,” a term that largely went out of use many years ago. But I would say no such thing exists for “family planning” except for those who see it as equivalent to “control.”
Q: I did not hear about the influence on culture on population growth. I think culture may explain the desire for children, especially in sub-Saharan Africa, and so it has made attitudes toward the use of contraceptives to control family size undesirable. How do you explain the thriving moments of family-size interventions against the cultural desire for children?
A: You are correct to say that cultural factors in sub-Saharan Africa favor large families; survey after survey verifies that. But family planning is more widely used among those with more schooling and who live in urban areas where larger families are less of an asset. That certainly suggests that the cultural factors can change, but at a national level that process is likely to be quite slow.
Q: One of the highest disparities is between rural and urban areas in SSA [sub-Saharan Africa]. With rising urbanization and increased temporary migration, can we expect this to continue to drive down fertility? Should we not encourage secondary education and delayed marriage in urban areas?
A: Certainly, rural-urban migration is a very significant contributor to reduced fertility. I’m sure you know about Ethiopia, where the total fertility rate (the average number of children per woman) in Addis Ababa was reported as 1.5 in the 2011 Demographic and Health Survey, but urban TFRs are lower in areas across sub-Saharan Africa. Secondary education should be expanded, and delayed marriage encouraged in both rural and urban areas, because rural populations will predominate for some time and are likely to grow more quickly.
Q: Other African countries not shown (e.g., Ethiopia, Rwanda, Mozambique) have lowered their TFR in the last decade even in the face of poverty and food insecurity. It is not just increased wealth and higher CPR [contraceptive prevalence rate], but also lowering under-5 mortality, urban residence, and the high cost of raising children. Can rising expectation, relative poverty + higher costs also drive down fertility?
A: It is remarkable how much infant and child mortality have declined in Africa. I have also wondered if that may be a precursor to reduced fertility. As you point out, fertility can definitely decline in high poverty countries and for the reasons you mention.
Q: What do you make of Deutsche Bank’s projection that the world population will peak at 8.7 billion in 2055 and only be 8 billion in 2100?
A: I have only glanced through that report but my impression is that it paints too rosy a picture by assuming that what has happened in some more rapidly developing countries will necessarily happen everywhere. There are large sociocultural, economic, and especially governance differences among countries that must be considered. It should always be remembered that population projections already assume that fertility will decline on a regular basis in all developing countries, which is far from certain. For the low figures offered by Deutsche Bank to be realized, even faster fertility decline would be required. That, I believe, is unlikely.
Q: Do you expect fertility to rebound somewhat in developed countries if the recession actually is ending?
A: There was little evidence of a fertility rebound even before the recession, so I don’t expect to see anything of significance after the recession ends. Only Russia has seen some rebound but that was due to the promise of large cash payments for the second and higher-order births, one case in which money actually “talked.” But so far in 2013, the rebound has begun drawing to a halt.
Q: Can you explain why TFRs are lower in Asia (e.g., Pakistan or India), than in Africa (e.g., Rwanda), yet CPR in Rwanda is either roughly the same as India or higher than Pakistan.
A: Excellent question! I think this is due to the predominance of temporary methods of contraception being used in Africa to space births rather than limit the eventual number. In India, female sterilization has always been the predominant method. If you look across Africa, the reported use of modern methods is unusually high compared to the high TFRs.
Q: Can we use world population data sheet in trend analysis?
A: I’m sorry, but since each data sheet is an update it can’t be used for times series. We have a note on the data sheet saying that. For example, TFRs are updated when new surveys are released and may be higher or lower than previous data sheets would suggest. The data sheet is quite useful for up-to-date figures, but for consistently derived time series, the UN Population Division’s biennial estimates and projections and the U.S. Census Bureau’s International Database are the obvious choices: United Nations Population Division: http://esa.un.org/unpd/wpp/index.htm and the U.S. Census Bureau: http://www.census.gov/population/international/data/idb/informationGateway.php.
Q: Is there a relationship between the total population size of a country and its fertility rate in the developing world?
A: No, there is no observable relationship between the two. India is the world’s second-largest country but has a total fertility rate (TFR) of about 2.4 while Niger has a population of 17 million but the continent’s highest TFR, at 7.6.
Q: Any thoughts on the impact of growing income inequality on fertility rates in the U.S.?
A: Well, the recent decline in the U.S. birth rate has been tied to the recession and the group most affected has been Hispanics, who do have lower income, particularly among more recent immigrants. So there could be some connection between lower income and fertility. According to the UN’s medium projection, the world would be close to 2.1 by 2050 but regions such as Africa still closer to 3.0. And a few other countries would still be above replacement, such as Iraq. However, it’s best to keep in mind that these are assumptions and not “forecasts,” if you will.
Q: If you ask me how many children are ideal after I have five children, I’m going to answer differently than if I have none. Therefore, I think the answers to ideal children is biased by the reality that many women already have a lot of children.
A: Yes, there can certainly be a bias based on the number of children respondents actually have. I mentioned in the webinar that the “ideal” children measure is somewhat subjective, I believe. There is another table in the Demographic and Health Surveys that shows the percentage of women by number of living children who do not want any more children. Comparing both gives a more complete picture.